 Trishna Pokhrel
Trishna PokhrelOroantral Communication and Fistula
- Oroantral communication is a pathological communication between the oral cavity and the maxillary sinus.
- An oral antral fistula is an epithelialized, pathological, unnatural abnormal communication between the oral and antral cavities.
Etiology:
- Oral fistula can result from following causes:
- Extraction of upper molars and premolar teeth (48%)
- Tuberosity fracture
- Destruction of the portion of the floor of sinus by periapical lesions.
- Implant dislodgement into maxillary sinus.
- Perforation of floor of sinus and sinus membrane. with injudicious use of instruments.
- Forcing of a tooth or a root into a sinus during its removal.
- Extensive trauma to face.
- Surgery of maxillary sinus.
- Osteomyelitis/ Osteoradionerosis.
- As a complication of the caldwell - luc surgery.
- Malignant granuloma
Predisposing Factors
- During extraction of post maxillary teeth.
- Hypercementosis or ankylosis of the tooth.
- Long standing decay or infected teeth.
- Severe Periodontitis.
- Previous history of oroantral communication.
- Density of the bone and the size of the sinus.
Symptoms of the Recently Created Oroantral Communication (5 E's):
1) Escape of fluid: Fluid regurgitation and escape of air through the nose from the sites of extraction.
2) Epistaxis: Unilateral epistaxis is seen due to escape of blood from the sinus the nose through the ostium.
3) Escape of air: Air escapes into the nose from the mouth during sucking, inhaling.
4) Enhanced column of air: Which causes a change in the vocal resonance and change in voice.
5) Excruciating pain: Severe pain in and around the region of affected sinus.
Sign of Recently Created Oroantral Communication:
- Disappearance of the root piece of the extracted tooth.
- Positive nasal blow test.
Symptoms Established Oroantral Fistula (Remember 5 P's)
1) Pain : As the fistula is established by epithellisation, it allows free escape of fluids, so pain is less then seen in early stage.
2) Purudent nasal discharge: When the head is lowered, there is persistent, purulent unilateral discharge from affected side of nostril.
3) Postnasal drip: Unilateral nasal discharge from the posterior nares, down the pharyme.
4) Possible sequence of general systematic toxaemic condition: Fever, anorexia, malaise, parietal and frontal headaches and in extreme cases, anosmia.
5) Popping out of an antral polyp: Opening of long-standing OAF is occluded by an antral polyp.
Signs of Established Oroantral Fistula:
1) Early Signs: Disintegration of blood dot as a result of forceful nose blowing, excessive mouth rinsing and infection. Signs and symptoms of sinusitis and rhinities.
2) Late signs: Escape of fluids on air through nose, development of polyps.
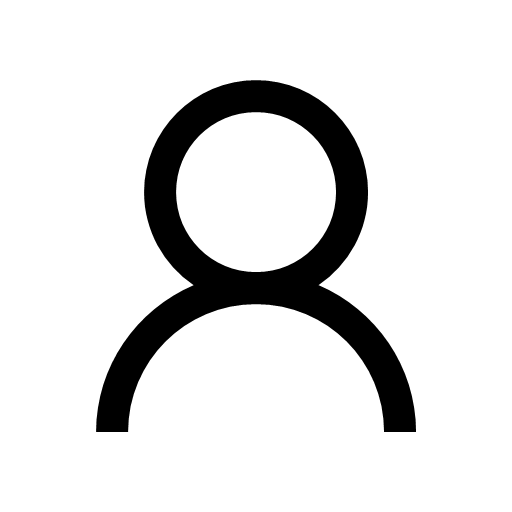
Decision Making in the Treatment of Oral antral communication and antral Fistula:
- if oral antral communication is less than 2 mm in diameter, without epithelialisation and in the absence of sinus infection, there can be spontaneous healing if proper precautions are taken.
- If the defects are larger than 5-6 mm spontaneous healing rarely takes place and will require surgical intervention.
Management of Acute Oroantral Fistula:
Temporary Measure:
1) Whitehead'sVarnish Pack:
- The pack is used over the socket and secured with sutures.
- Whitehead's varnis:
- Benzoin 10 parts 44g
- Storax 7.5 parts 33g
- Balsam of Toke 5 parts 22 g
- Iodoform 10 parts 55 g
- Solvent ether to 1flO2 O2 100 parts
2) Denture Plate:
- Indicated with there is delay in surgical repair of fistula. Denture plate acts as barrier to prevent entry of food particles into the antrum.
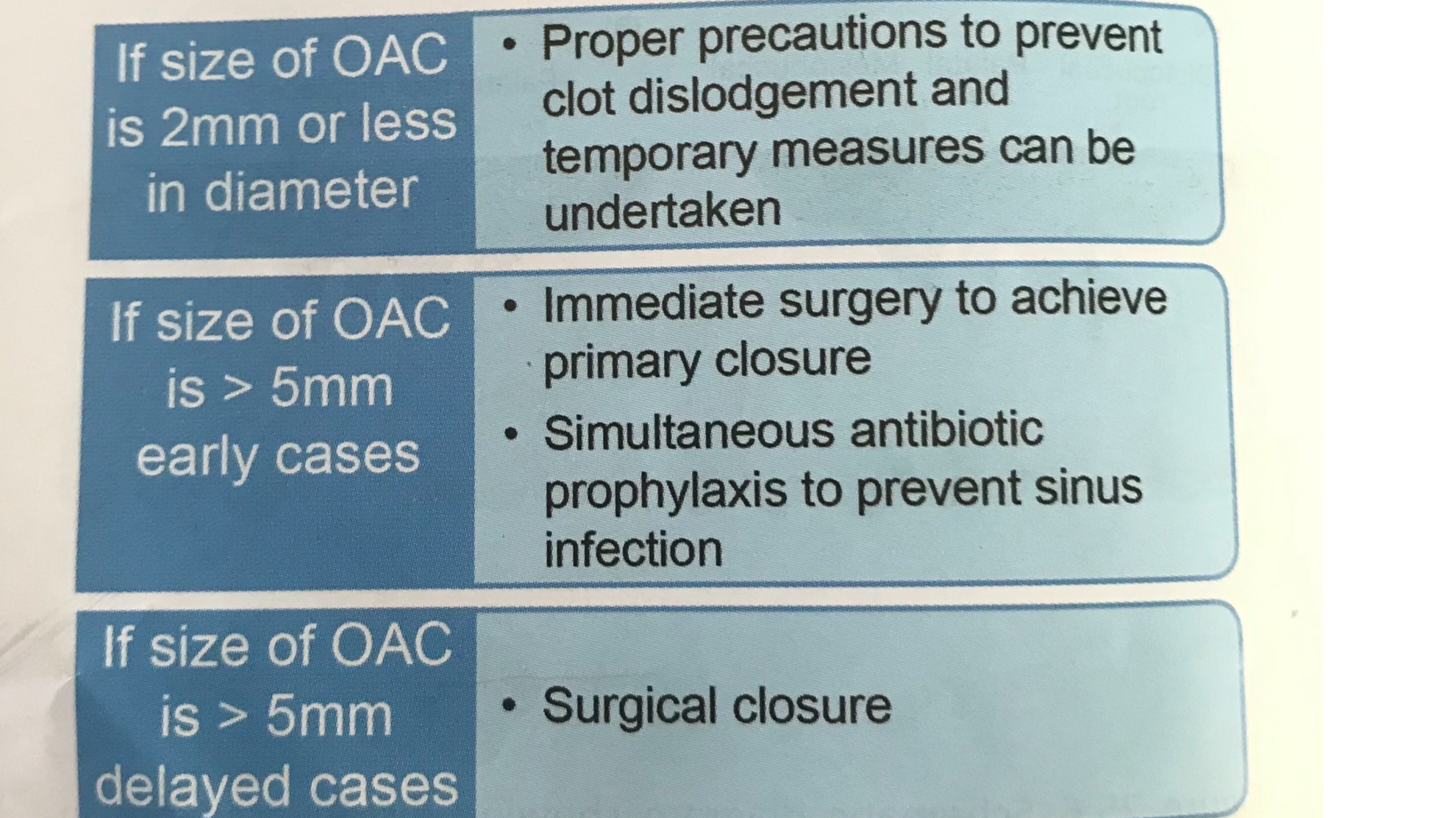
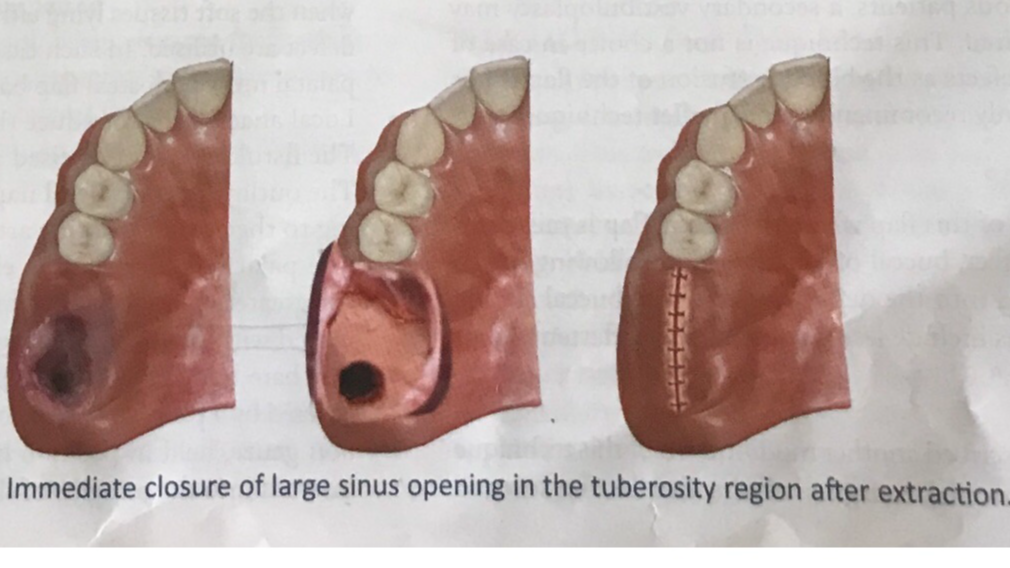
Immediate Closure:
- Primary closure of the socket by mucoperiostal flops, is the simplest method which is obtained by reducing the height of the bony socket.
- Antibiotics are prescribed to prevent sinus infection.
Supportive Measure:
- Antibiotics: These are preserbed to prevent secondary infection at the site, to prevent pre existing infection of antrum.
- Based on culture and sensitivity testing, the selection of antibiotic must be done.
Penicillin and its derivatives:
- Initially i.v route and later switched to oral route.
- Penicillin V 250 - 500 mg six hourly.
Nasal Decongestants:
The encourage the drainage of pus and secretions. for e.g. Ephedrine(0.5 %) or otrivin nasal drops 3 drops TDS for 7 days.
Analgesics: NSAIDs
- Tablet Aspirin 500 mg OID daily.
- Tablet paracetamol 500mg TDs daily.
- Tablet Ibuprofen 400mg TDS daily.
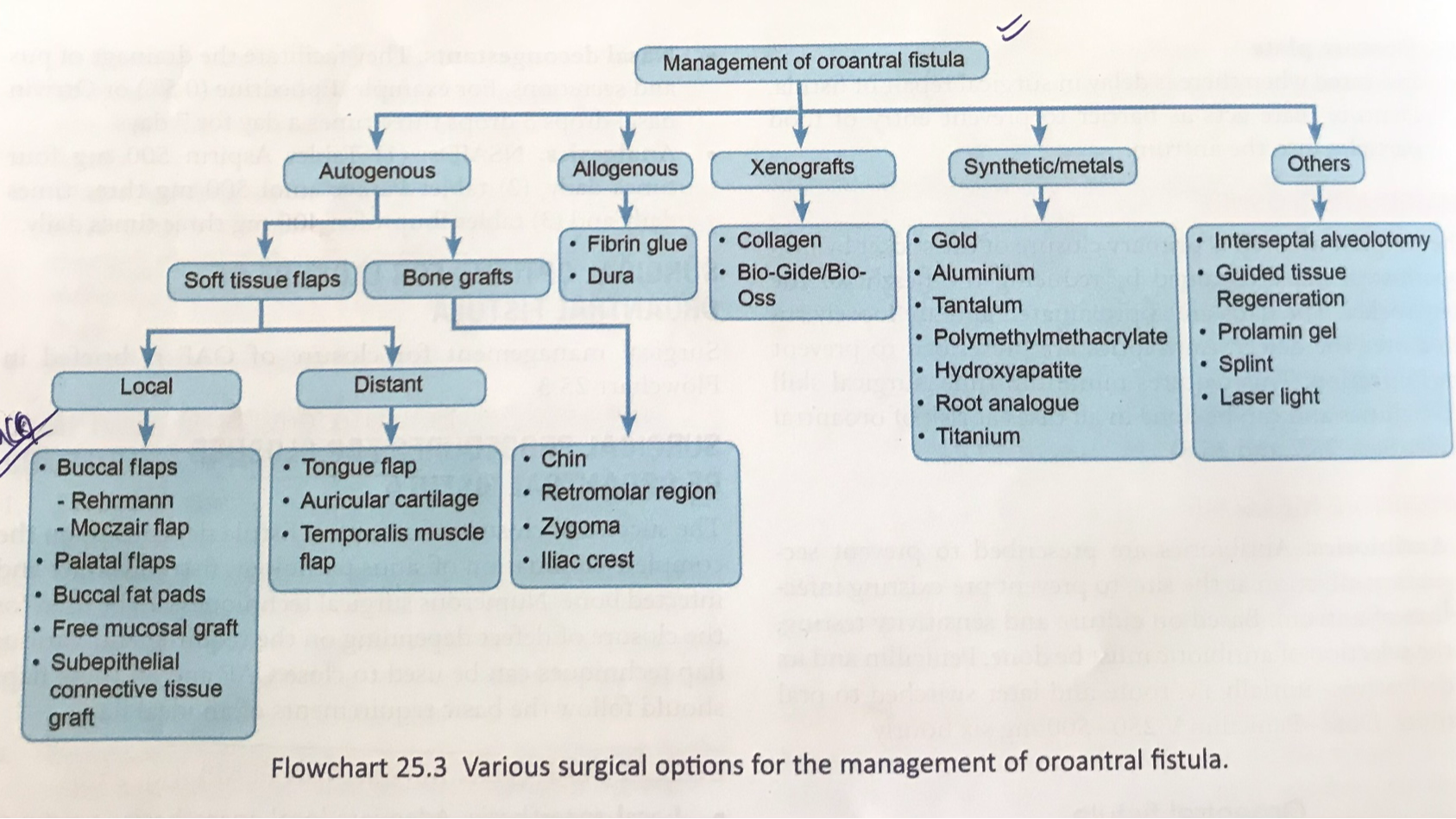
Surgical options for closure of oroantral fistula.
Surgical management for closure of OAF is briefed in flowchart.